Categories
A case of incomplete pentalogy of Cantrell in “Bo” the Border Collie.
By Gerard Olivares and Robert Weekes
History and physical examination
A 4-year-old male neutered Border Collie named Bo was presented to his first opinion veterinary practice with a week’s history of lethargy, exercise intolerance, weight loss, intermittent vomiting, and polyuria and polydipsia (PU/PD). Investigations included blood work, namely complete blood count (CBC), serum biochemistry, coagulation times, vitamin B12, folate, TLI and cPL, and abdominal ultrasound. These investigations revealed a stress leukogram, mildly increased basal bile acids, increased alanine transferase (ALT 390 U/L, RI 0-100), apparent microhepatica and absent gallbladder. Bo received amoxicillin/clavulanic acid and ursodeoxycholic acid and was referred to the Internal Medicine Service here at Eastcott Veterinary Hospital. The only relevant previous medical history was an umbilical hernia repair at 6 months old. Bo was very bright and alert on physical examination. There had been a 10% weight loss and the body condition score was decreased (BCS 3/9). The xiphoid process was absent on palpation.
Problem list and differential diagnoses:
While Bo presented with several problems, some such as weight loss, exercise intolerance or intermittent vomiting are unspecific and carry a multitude of differential diagnoses. The more relevant and specific problems in this case were the increase in ALT, absent Xiphoid process and previous umbilical hernia (table 1).
Table 1:
| Problem List | Differential Diagnoses |
| Increased serum ALT | Primary hepatic disease (eg, hepatitis), endocrinopathies, reactive hepatopathy (e.g. gastrointestinal disease), infectious diseases, hypoxia and neoplasia. |
| Absent Xiphoid process and umbilical hernia | Congenital anatomical defects, trauma. |
Diagnostic Investigations:
At the referral consult a CBC was performed indicating a mild lymphopenia and was otherwise unremarkable. Serum biochemistry revealed increased but stable ALT levels. Bo’s gastrointestinal signs and concurrent PU/PD meant that Hypoadrenocortism was possible. An ACTH stimulation test was performed, and this ruled out hypoadrenocorticism.
An abdominal ultrasound demonstrated a ventral mid-line diaphragmatic defect with herniation of the stomach, proximal duodenum, the spleen, the pancreas, and a portion of the liver including the left lobes and the gall bladder (figure 1).
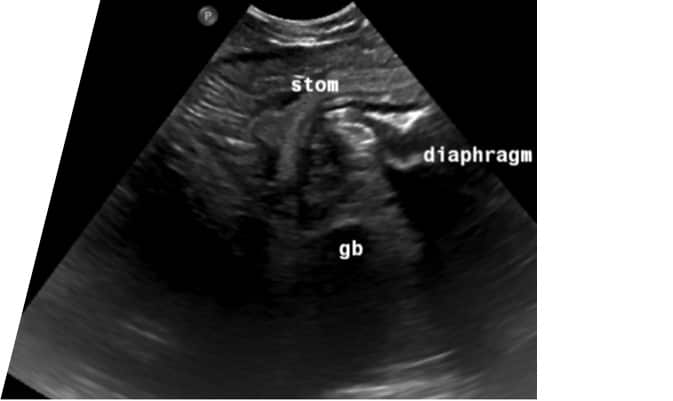
Figure 1; Frozen image of ultrasound scan showing herniation of stomach and gall bladder through the diaphragmatic defect.
Due to the findings on the abdominal ultrasound, it was decided to perform a CT scan to further characterise the diaphragmatic defect and precisely locating all displaced viscera. On CT scan a large 4cm defect was discovered in the diaphragmatic midline slightly caudal the foreshortened and abnormally shaped sternum (Figure 2). The spleen, gall bladder, pancreas, pyloric antrum, and proximal duodenum were all herniated through this defect and likely sitting within the pericardial sac surrounding the heart ventrally, confirming a diagnosis of Congenital Peritoneopericardial Diaphragmatic Hernia (cPPDH). Although not featured highly on our differential list cPPDH is a recognised congenital defect that often involves herniation of organs into the pericardial space. Due to its nature as a congenital condition, it is often diagnosed early in a patient’s life, but, as occurred in this case, some dogs can live with a cPPDH for several years with no obvious clinical abnormalities. In this patient we believe the presenting signs (lethargy, exercise intolerance, weight loss, intermittent vomiting, and PU/PD) were due to the visceral pain or nausea caused by herniation of abdominal visceral through the diaphragmatic defect. An increase in ALT is a common laboratory finding in both cats and dogs with cPPDH, supposedly caused by trauma to the liver, as previously described in the literature. (Banz & Gottfried, 2010). The combination of diaphragmatic, pericardiac, body wall and sternal defects makes this a likely case of incomplete pentalogy of Cantrell (Benlloch-Gonzalez & Poncet 2015, Williams et al. 2020).
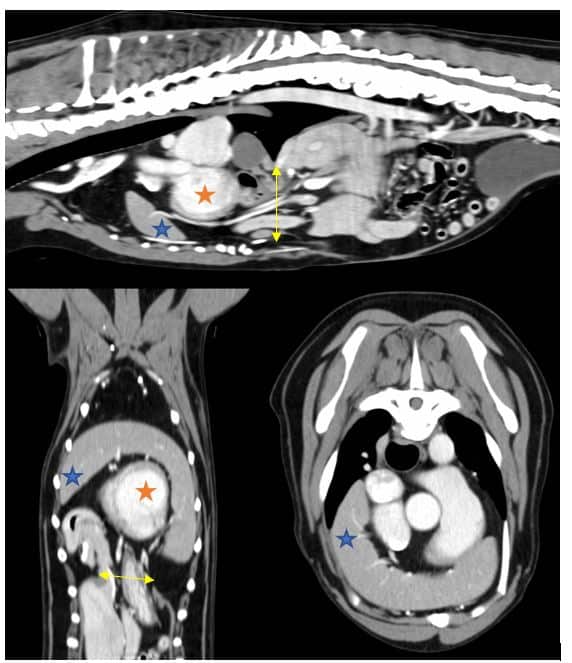
Figure 2; Three CT scan views of the thorax showing herniated viscera extending through the diaphragmatic defect (indicated by yellow arrow) into the pericardial sac. The spleen (indicated by blue star) can be seen extending around the cranial border of the heart (indicated by orange star).
Treatment Options and Prognosis:
Both conservative and surgical options can be considered in the treatment of cPPDH cases. A 2013 publication looked at the outcomes for dogs and cats with PPDH which received both treatment options (Burns et al., 2013). It was found that there was no significant difference in long-term survival time between treatment options, but that a larger proportion of cases with clinical signs attributable to the defect, as there were in this case, went on to be surgically managed. This publication also showed that the rate of surgical complications was low and the long-term prognosis for resolution of clinical signs was good. Since Bo had clinical signs, that could be attributed to the cPPDH, and were progressive surgery was recommended.
Surgery:
Bo underwent surgical management of the diaphragmatic defect and herniated abdominal viscera. A midline coeliotomy was performed and the peritoneopericardial hernia was confirmed, alongside herniation of the spleen, gall bladder and quadrate liver lobe. The quadrate liver lobe and gall bladder were easily reduced with gentle traction; however, the spleen was irreducible. A caudal median sternotomy of the two most caudal sternebrae was performed to improve visualisation and access to the herniated spleen. An omental adhesion between the spleen and the cranial pericardium was identified and was preventing reduction of the spleen. On further inspection, the omentum was found to be herniated through an additional defect in the midline of the cranial pericardium and was adhered to the cranial mediastinal structures. A vessel sealing device was used to release the omental adhesion and the spleen was successfully reduced. The caudal sternum was closed with 0 polydioxanone (PDS) figure of eight sutures. The diaphragmatic defect was closed with 2-0 PDS in a simple continuous pattern and air was drained from the pericardium via thoracocentesis. The abdomen was closed routinely, and the patient recovered in our intensive care unit.
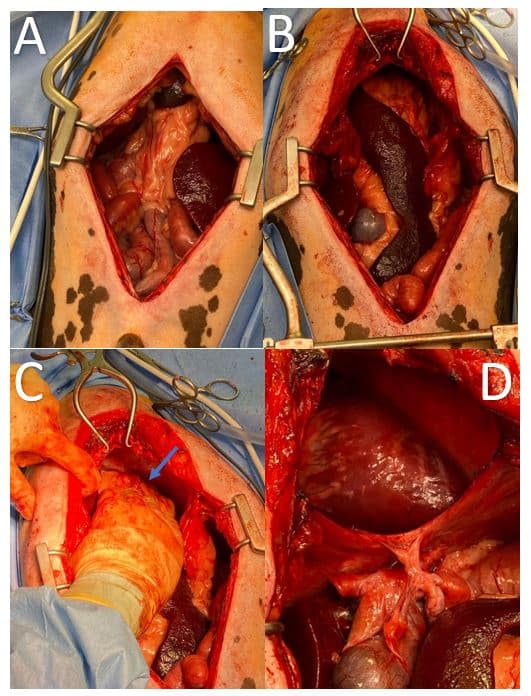
| Figure 3: Intraoperative photos; A) Midline coeliotomy showing herniated abdominal viscera extending cranial into the pericardiumthorax. B) Improved exposure after caudal median sternotomy, showing spleen and omentum extending through the diaphragmatic hernia into the pericardium. C) Caudal retraction of the spleen and omentum revealing an adhesion through the defect within the cranial pericardium (indicated by blue arrow). D) Thoracic cavity after removal of the herniated abdominal viscera. |
Outcome:
Following an uneventful recovery, Bo was discharged three days post-surgery for strict rest at home for four weeks postoperatively. At follow up at four months post-surgery the patient was reported to be exercising at a level greater than before presentation and had a much better appetite. There were no other concerns.
Conclusion:
cPPDH is a rare condition which can present with vague/non-specific clinical signs in young and adult dogs. Diagnosis is made through imaging of the abdominal and thoracic cavities by radiographs or ultrasound; however, CT scan can be helpful at achieving a definitive diagnosis and can be useful for surgical planning. Although research has shown that there is not a significant difference in the outcome for patients who undergo surgery (Burns et al., 2013), in some cases, the improvement in clinical signs seen with surgical resolution of the hernia, show that it can be a viable option for the management of a cPPDH. During our research for this case, we found that the combination of midline congenital defects can be grouped together into the pentalogy of Cantrell, a well-documented condition in human medicine, and is made up of five congenital defects affecting the sternum, midline abdominal wall, heart, diaphragm, and pericardium. In our case there were four of these defects found which therefore makes this a case of incomplete pentalogy of Cantrell.
Acknowledgments:
I’d like to give my thanks to the entire team at Eastcott Veterinary Referrals for their involvement in this case and especially to Gerard Olivares and Charlotte Howes for their help in producing this case report. Finally, I would like to thank Bo’s owners for consenting to sharing details of the case.
References:
Banz, A. C., & Gottfried, S. D. (2010). Peritoneopericardial Diaphragmatic Hernia: A Retrospective Study of 31 Cats and Eight Dogs. In J Am Anim Hosp Assoc (Vol. 46).
Benlloch-Gonzalez, M., & Poncet, C. (2015). Sternal Cleft Associated with Cantrell’s Pentalogy in a German Shepherd Dog. Journal of the American Animal Hospital Association, 51(4), 279–284. https://doi.org/10.5326/JAAHA-MS-6181
Burns, C. G., Bergh, M. S., & McLoughlin, M. A. (2013). Surgical and nonsurgical treatment of peritoneopericardial diaphragmatic hernia in dogs and cats: 58 cases (1999–2008). Journal of the American Veterinary Medical Association, 242(5), 643–650. https://doi.org/10.2460/javma.242.5.643
Williams, P., Booth, M., & Rossanese, M. (2020). Incomplete pentalogy of Cantrell in a Border terrier puppy. Veterinary Record Case Reports, 8(4). https://doi.org/10.1136/vetreccr-2020-001188