Categories
Bronchoscopy in Bronchial Foreign Body Removal in Dogs
Bronchial foreign body
Bronchial foreign body is a differential diagnosis in dogs presenting with a history of an acute or chronic cough. Most bronchial foreign bodies are located within the right bronchial ramification and have a tendency to move deeper or migrate throughout pulmonary parenchyma to surrounding tissues and organs. About 30% of bronchial foreign bodies can be missed using the radiography for detection. At present thoracic CT and bronchoscopy seem the most sensitive diagnostic modalities, later allowing also the removal of the foreign body. Bronchoscopy was demonstrated to be useful in removing foreign bodies despite the size of the animal and the duration of clinical signs. It also presents an excellent non-invasive alternative to surgical management..
History
The patient was a 3 year old, male neutered SBT cross with a 3 week history of chronic productive coughing, lethargy and partial anorexia. Several chest radiographs were taken which did not show any significant abnormalities. Blood results were unremarkable and faecal examination negative for lungworms. Bronchoscopy was performed and a foreign body at the level of the right main stem bronchus was found. The foreign body could not be removed during the bronchoscopy so the dog was started on antibiotic therapy and referred to our hospital.
On presentation to the internal medicine department
On physical examination the dog was calm, febrile (39.5°C) and coughed several times during the examination. The rest of the physical examination was unremarkable.
Further diagnostics and treatment
In order to evaluate the exact location and the size of the foreign body and aid decision-making (medical or surgical management), a CT was performed revealing foreign body at the level of the right main stem bronchus. Bronchoscopy was performed and prior to foreign body removal, the non-affected and the affected airways were thoroughly examined and a BAL performed.
Multiple foreign bodies were successfully removed (grass awns/seeds). Due to pronounced regional swelling of the tissue and the presence of large amounts of mucopurulent discharge a thorough examination of the affected site for further foreign bodies and to evaluate the extent of the local site inflammation, was not possible.
Bronchial washes were sent for cytological examination, culture and sensitivity. Results indicated purulent inflammation although no bacteria were present on cytology slides or cultures. Antibiotics were continued and the dog was discharged after 4 days of hospitalisation.
The dog was re examined 2 weeks after discharge and was found to be generally well and the frequency of coughing substantially decreased but was still present. Physical examination was unremarkable. Given the disseminated nature of the foreign body and the fact that post removal detailed examination of the affected site was not possible, a control CT was performed. No foreign bodies were detected but local inflammation and local dilation of affected bronchus remained. Antibiotic treatment was extended for 2 weeks and the dog is currently scheduled for a repeat examination.
Fig 1
Bronchial Foreign Body

Fig 2
CT image of the bronchial foreign body with the surrounding localized bronchopneumonia
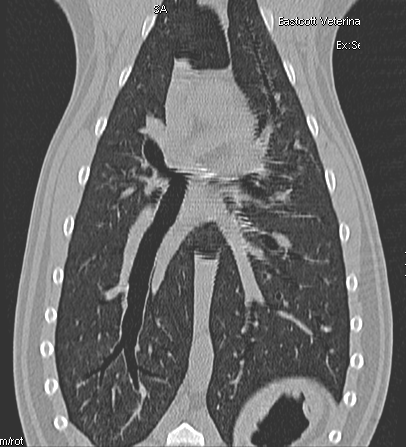
Fig 3
CT image at 2-week re examination
If you think you have an Internal Medicine case that you would like to refer or discuss. Please phone 01793 528341 or contact Internal Medicine