Categories
Immediate Mandibular Bone Reconstruction in a Dog
Immediate Mandibular Bone Reconstruction Following Segmental
Mandibulectomy in a Dog
 with Peter Southerden
with Peter Southerden
Mandibulectomy is a recognised and commonly used technique to treat a variety of mandibular tumours and severe mandibular trauma. Significant bone defects after segmental mandibulectomy allow mandibular drift towards the side of the resection resulting in malocclusion, difficulty in eating and temporomandibular joint pain. Though segmental mandibulectomy without reconstruction produces acceptable and functional results in almost all cases I believe that there are clear benefits to jaw reconstruction where this is possible.
Herbie was an eight year old neutered male cross breed dog that presented to Eastcott Referrals for the treatment of a canine acanthomatous ameloblastoma affecting the right mandible at the level of the second mandibular molar.
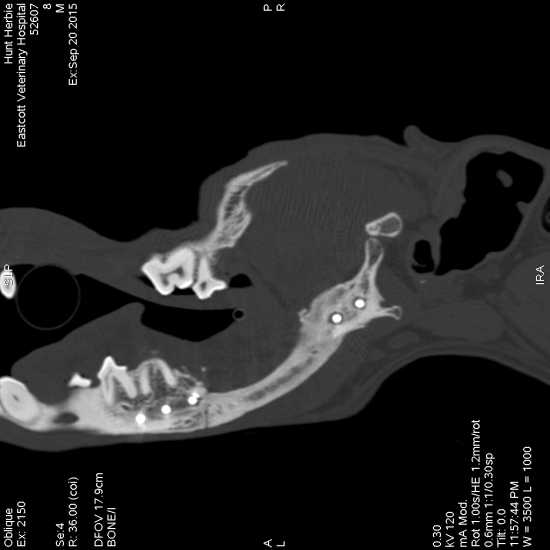
A CT scan was performed which allowed accurate assessment of the limits of tumour invasion and consequent surgical margins
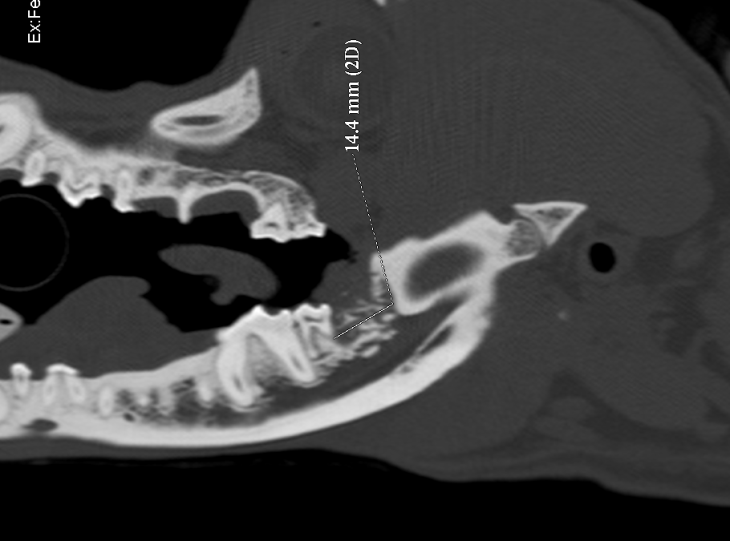
Sagittal view of a CT scan showing the presence of an invasive mass at the level of the right second mandibular molar in a dog
These were drawn onto a sagittal view of the affected mandible allowing detailed preoperative planning of the resection.
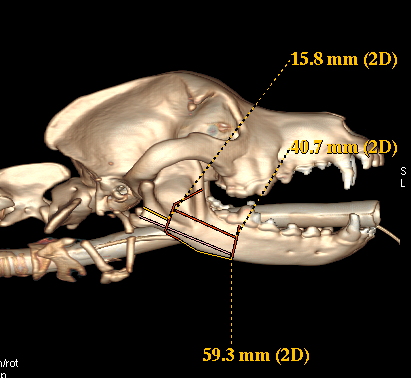
Right lateral view of a three-dimensional reconstruction of a CT scan of the skull of a dog showing measurements taken for surgical planning to ensure a 1 cm surgical margin for resection of an acanthomatous ameloblastoma.
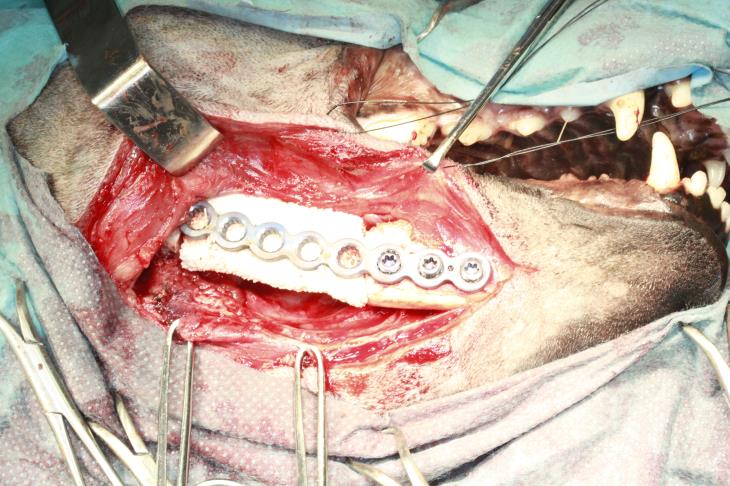
Preoperatively a 10mm cuffed tube was placed using a transmyelohyoid approach and secured with finger-trap sutures to allow unimpeded access to the oral cavity. The mandible was initially accessed by an extraoral approach and the margins of the resection marked. A ten hole 2.7mm PAX locking plate (Securos, UK) was then contoured to the mandible and fixed with two locking screws caudal to the proposed resection and three rostral. The plate was then removed and the surgical approach temporarily closed.
The mandible was then accessed via an intraoral approach and the tumour resected precisely according to the predetermined margins using a piezotome bone saw (Piezotome Solo – Acteon) and the oral wound was closed in two layers. The bone plate was then replaced via the extra-oral approach and secured in place with four 10mm and one 8mm locking screw. A template was made to fit the defect precisely and this was used to cut a compression resistant bone grafting matrix (Master Graft Strip, Medtronic, Hertfordshire, UK) to the correct size. The CRM (compression resistant matrix) was then infused with 1.32 mg of rh-BMP (TruScient – Zoetis) in 2.8ml of saline and placed in the defect and sutured circumferentially to the bone plate with poliglecaprone-25 to prevent movement of the graft. The extra-oral incision was then closed carefully in three layers
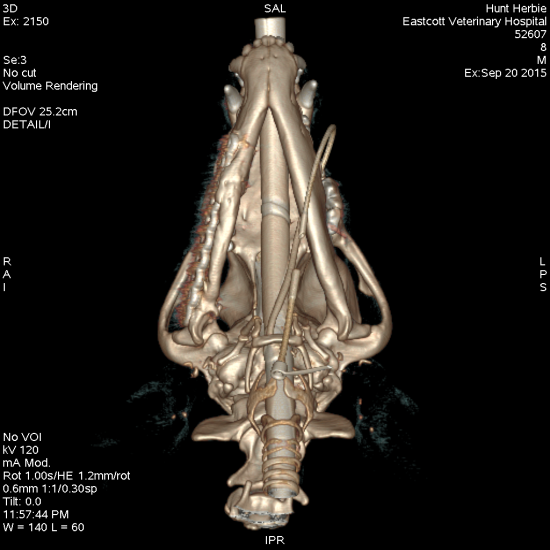
Herbie had excellent occlusion postoperatively and throughout his follow up period. Hard tissue spanning the defect was palpable and evident on CT examination at six weeks and this had increased to more substantial bone repair at six months postoperatively. The owner reported that Herbie had returned to normal function and had an excellent quality of life.
I believe that the result of this procedure was considerably better in terms of recovery, comfort and function compared to a resection without reconstruction and would be very happy to discuss this with referring veterinary surgeons who have patients for whom this might be a suitable procedure.
Peter and the Dentistry Referral team are happy to offer his advice on dentistry and oral surgery cases