Categories
Nasal SCC and Sentinel Lymph Node Identification in Dog
Sentinel Lymph Node Identification in a Dog with Nasal Squamous Cell Carcinoma

Cadbury is a 10-year-old Labrador who initially presented with a small ulcer on his nasal planum. This gradually enlarged until Cadbury had a large proliferative and erosive mass (Fig.1). A histological biopsy was taken confirming a diagnosis of Squamous Cell Carcinoma (SCC).
Nasal SCC is the most common malignancy diagnosed affecting the canine nasal planum. It is characterised by being locally invasive whilst also having the potential for metastases to the draining lymph nodes and lungs. Many cases are amenable to resection but this is often declined by owners as any resection of the nasal planum will fundamentally alter the appearance of the dog and this is very hard for many owners to come to terms with. It is therefore imperative that cases are adequately staged prior to surgery to avoid any dogs undergoing this type of invasive surgery unless there is a good chance of cure or at least a reasonable period of remission.
SCC can spread to the draining lymph nodes but the size alone of these lymph nodes is sadly not enough to determine whether or not any metastasis has occurred. Many cases of metastases can be detected using ultrasound-guided aspiration of these nodes but there is still a significant risk of either a false-negative or even a false-positive result. The gold standard is, therefore, histological evaluation of the draining lymph nodes with extirpation of multiple lymph nodes (e.g. submandibular, parotid and retropharyngeal) usually being recommended to adequately stage a solid neoplasm of the head.
There has been a considerable drive in human surgery to identify the main draining lymph node to a specific tumour site. This lymph node is termed the Sentinel Lymph Node (SLN) and analysis of the SLN should indicate the true stage of the tumour without the need to take out multiple lymph nodes which is associated with considerable morbidity (e.g. lymphedema) in people. Recent work in veterinary patients has shown that similar techniques can be employed. Sometimes the SLN is not the nearest or seemingly most logical lymph node and can be surprisingly distant from the tumour being assessed.
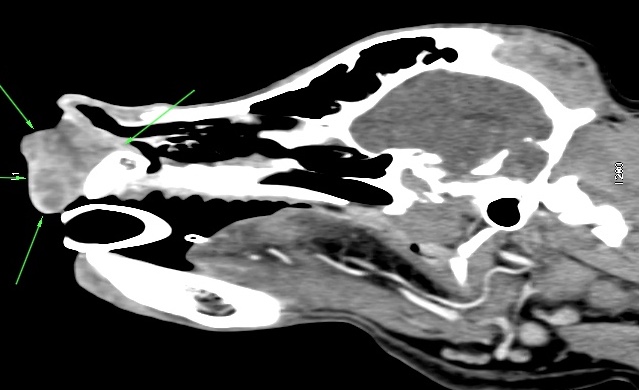
Cadbury had his tumour staged using Computed Tomography (CT) scans. In addition to conventional CT which showed the local extent of his nasal tumour (Fig. 2) and excluded overt pulmonary metastases, multiple enlarged lymph nodes were seen. These lymph nodes may have been enlarged due to either metastases or lymphoid reaction to the inflammation associated with the mass.
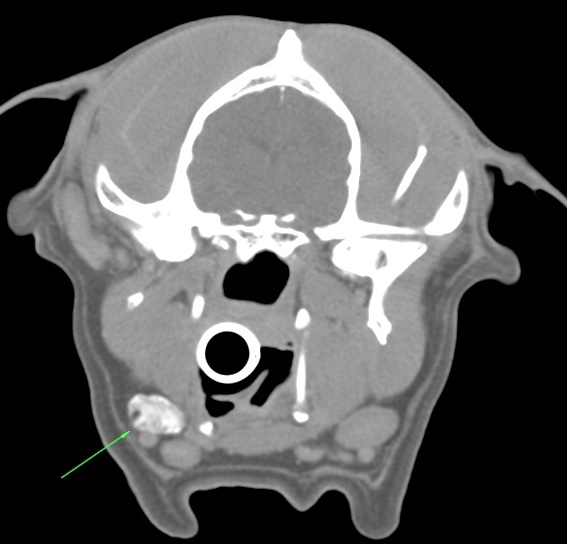
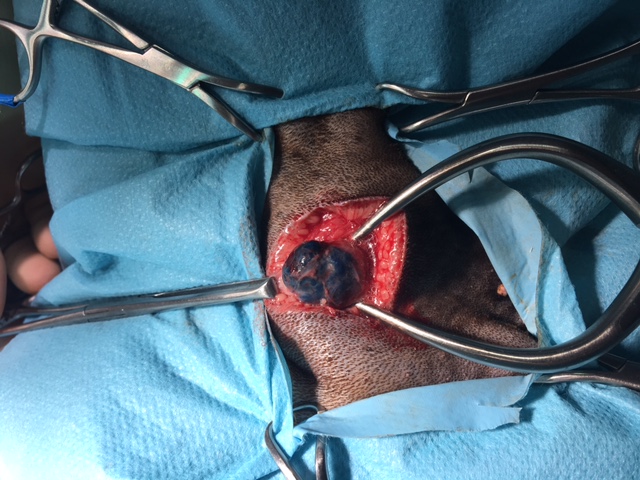
Peritumoral injection of contrast agent was then used as a type of indirect lymphography. In Cadbury’s case, the lymphatics could be traced from the tumour site to one of the submandibular lymph nodes which were therefore identified as the SLN (Figure 3). Peritumoral vital dye was then injected and Cadbury was taken to theatre where the dye had drained along the lymphatics to colour the SLN blue aiding its identification (fig 4).
Fortunately, Cadbury’s SLN was clear of metastases and so he was later taken to surgery where his nasal planum was resected en-bloc with a rostral maxillectomy. Surgery went well, a modified technique was used which involved rotating the rostral labial tissue dorsomedially to reconstruct a nasal philtrum and to create a nasal vestibule which is more cosmetic than the older techniques of simple excision and mucosal-skin apposition. A clean margin of excision was achieved and Cadbury is now recovering well.

Figure legends:
Figure 1: Preoperative appearance of erosive nasal SCC
Figure 2: coronal CT showing local extent of tumour
Figure 3: Indirect lymphographic CT showing contrast enhancing SLN
Figure 4: SLN stained blue allowing easy identification
Figure 5: Postoperative appearance following en bloc SCC resection with rostral maxillectomy