Categories
Traumatic Injuries to Juvenile Teeth in Dogs

The eruption of the secondary, or permanent, dentition occurs between 12 weeks and 28 weeks in dogs. The first teeth to erupt are the incisors and the last the molar teeth. On completion of eruption the crown of the tooth is fully formed and will not change for the remainder of the dog’s life unless an external force is applied. This does not apply to the root of the tooth.
Once mature the tooth is essentially a hollow tube closed at both ends with perforations at the root tip to allow neuro-vascular tissue to enter which in combination with fibrous stroma and odontoblasts form the pulp tissues. Odontoblasts deposit dentin on the internal surface of the root progressively throughout life. This continued deposition can be used as a marker of pulpal vitality as asymmetry in root canal diameter between contralateral teeth, or unchanged diameter between the same tooth at different times indicates pathology.
At the time of eruption, the root of the tooth is immature. The root develops from the crown end towards the tip of the root but at the time of eruption the thickness of the dentin tapers from the crown rapidly to an egg shell thickness and the root tip is not formed. The root reaches its final, mature anatomy between 9 and 15 months of age, depending on the tooth.
The canine teeth and the maxillary 4th premolar and mandibular 1st molar teeth are considered to have strategic importance. The loss of these teeth has implications for an individual’s long-term quality of life and extraction is an invasive procedure and associated with significant potential complications. Of course, loss of teeth may be unavoidable and these patients will adapt, once recovered from treatment, but there may be options to preserve these teeth with appropriate action.
Fracture of teeth is common in dogs and can be broadly defined as either complicated, directly exposing the pulp, or uncomplicated involving the enamel and dentine only. Exposure of the pulpal tissues to the microflora of the oral cavity will result in bacterial colonisation of the pulp and its subsequent death. The root canal following plural necrosis is a privileged environment for these bacteria due to the inability for an effective immune response to be mounted. Eventually, the inflammatory mediators and bacteria will cause a peri-apical periodontitis which may progress to a true apical abscess, granuloma or radicular cyst. Uncomplicated fractures can also result in colonisation of the pulp by migration of bacteria along the exposed dentinal tubules. The closer the fracture to the pulp the greater the potential for pulpitis and therefore this is more common in younger patients as the dentin is less thick than older individuals. Following a complicated crown fracture, bacterial colonisation of the pulp is rapid and an irreversible pulpitis and subsequent pulp necrosis is likely to occur within 7 days from the time of pulp exposure.
Preservation of endodontically challenged teeth may be achieved through root canal treatment. The success of root canal treatment is reliant on elimination of bacteria from and the subsequent sealing of the root canal. This is not possible if the root is not fully formed as in the case of immature teeth and thin dentinal walls of these immature teeth are unlikely to be able to stand the rigours of life. Preservation of immature teeth is reliant on the preservation of the vitality of the pulp to allow for continued maturation of the root. Success rates for the maintenance of pulp vitality is at its highest within 48 hours of pulp exposure and if treated appropriately 92% of teeth are reported to remain vital for the length of the patient’s life. As a result, a complicated crown fracture of an immature tooth must be considered as an emergency.
The treatment used for preservation of immature fractured teeth is referred to as a Vital Pulp Therapy. This involves amputation of the most coronal part of the pulp and placement of dressing material directly onto the pulp and then restoration of the fracture to prevent ingress of bacteria. The dressing material allows dentin deposition at the cut surface of the pulp forming a dentinal bridge further sealing the pulp. Follow up dental radiographs are important to monitor the continued vitality of the tooth and these are routinely performed at 3 and 18 months after treatment.

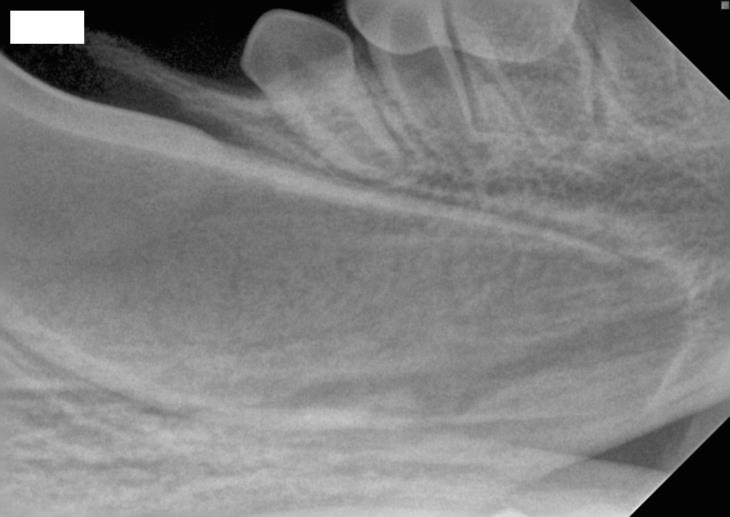

Fig 1: Fractured tooth with pulp exposure.
Fig 2: Radiograph of immature tooth root, the root canal is extremely wide, the dentinal walls thin and there is no formed root apex.
Fig 3: The same tooth seen in Image 2 four months after treatment indicating continued development of the root.
If you have an urgent case that you wish to discuss the Dentistry Team at Eastcott Referrals are happy to be contacted directly by telephone or email